
Heterogeneous
The One Word That Could Change Your Cancer Treatment
A look at the proposed metastatic triple-negative breast cancer algorithm—and why understanding your tumor's biology may be just as important as understanding your diagnosis.
"Girl… I'm hiding HER2-low." That was the sassy voice I gave to my little cardboard, cutout, co-host, named Heterogeneous, (the featured thumbnail picture, with me above at a event, she’ll be making special appearances in future content) as I prepared to record a video over the holiday weekend. It made me laugh, but then I realized something, she's right. Cancer does hide things, and sometimes those hidden clues can change everything. That's exactly what heterogeneous means. It reminds us that cancer is rarely one-size-fits-all. Every tumor has its own biology, and understanding that biology opens the door to more personalized treatment options. Having the ability to do so, saved my life. It provided me with an opportunity, very early on in my metastatic treatment journey, that otherwise would have been overlooked. Some call it fate, some call it God’s will. Some say I am a miracle, while others say I’m solutions driven, a case study in resilience. Say what you want but the word that is often overlooked in the patient community is: Heterogeneous - The One Word Every Metastatic Breast Cancer Patient Needs to Know. In plain English, heterogeneous simply means "not all the same."
The word “Cancer” equals hundreds of different diseases. In Triple Negative Breast Cancer there are currently between 4 to 6 distinct molecular subtypes (1)(subsets) according to the ASCO Educational book published in April of 2026. Identifying your subtype takes away the “one size fits all” concept and uses heterogenous as the key concept, providing personalized treatment options, based on your subset or tumor micro environment. The label is only the beginning, the biology is the real story. That is what scientists mean when they describe cancer as heterogeneous.
A New Treatment Algorithm Brings New Hope
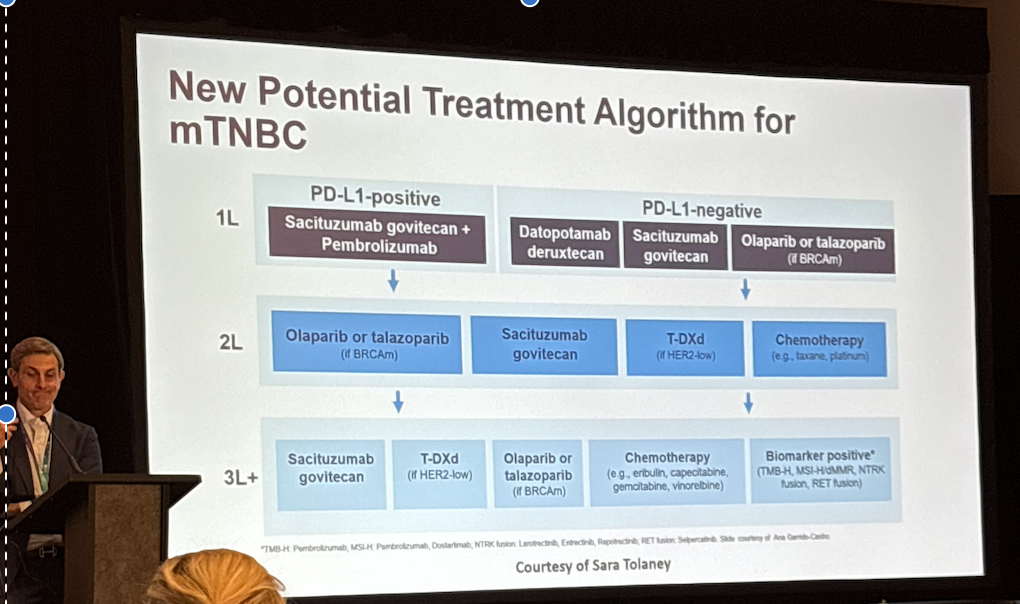
*presentation slide of new proposed mTNBC treatment algorithm ^
During CURE’s Patient Educated Breast Cancer Summit, at the Miami Breast Conference in March of 2026 I learned that a new proposed treatment option for mTNBC was being introduced. Immediately my curiosity was raised as a decade long survivor (given just a 4% chance) whose life was extended due to my participation in clinical research. It was exciting. For the first time, I could see how much progress has been made. Patients now have access to immunotherapy, antibody-drug conjugates, PARP inhibitors, HER2-low therapies, and biomarker-directed treatments that simply didn't exist when I was diagnosed. But as I looked at the slide, one question kept coming back to me. How do we know a patient is entering the right pathway (treatment option) if we haven't fully understood the biology of their cancer? An algorithm is only as good as the information that feeds it, and that information starts with biomarker testing.
Biomarker Testing Saved My Life
When I was diagnosed with metastatic triple-negative breast cancer in 2017, I was fortunate & savvy enough to fight for a spot on an innovative clinical trial. At the time, I became the first patient in the country with metastatic triple-negative breast cancer to receive the combination of NKTR-214 (bempegaldesleukin) and nivolumab (Opdivo) in the PIVOT-02 trial. Neither drug has been approved to target mTNBC, but that is the miraculous, beauty of my story.
Through today's scientific lens, I believe the biomarker testing helped identify an immune-responsive tumor microenvironment that made me a strong candidate for that clinical trial. While we can never know with certainty why one patient responds and another doesn't, I often wonder, but am pretty much convinced that understanding my biology early on and the value of making an informed decision, gave me an opportunity I otherwise might never have had. The benefits can look like remission, which I’ve been in officially since 2020!
Looking back, I realize something.
It wasn't just the drugs that changed my life.
It was the decision to look deeper.
My tumor belonged to an immune-responsive subset. Today we understand much more about the importance of the tumor microenvironment and the interaction between cancer cells and immune cells in determining who may benefit from immunotherapy. If no one had explored those possibilities, early on, if my biology had never been investigated, I may never have reached the treatment that ultimately gave me the opportunity to become a long-term survivor.
Then I Heard Something That Changed My Thinking
A physician recently said something that has stayed with me.
"The report is the diagnosis."
At first I wasn't sure what he meant.
Then it clicked.
The pathology and genomic reports don't simply confirm cancer.
They reveal its biology.
They identify biomarkers.
They uncover treatment opportunities.
The report isn't just paperwork.
It's the roadmap.
The Equity Gap We Can't Ignore
Unfortunately, not every patient has equal access to biomarker testing, genomic sequencing, or referral to clinical trials. According to the 2026 AACR Cancer Disparities Progress Report, that reality disproportionately affects underserved communities (2), including many African American patients. As a patient navigator, I have spoken with individuals who had never heard the words biomarker testing until months—or even years—after diagnosis.
Some didn't know the testing existed.
Others assumed if their doctor didn't mention it, it must not matter.
But knowledge is part of access.
And access saves lives.
Before Your Next Treatment Decision
Don't be afraid to ask:
Have all of my recommended biomarkers been tested?
Should we repeat testing if my cancer has changed or progressed?
Can I see my pathology and genomic reports?
What do these results mean for my treatment options?
Are there clinical trials based on my biology—not just my diagnosis?
Because your diagnosis is where the conversation starts.
Your biology is what helps guide where it goes next.
Final Thoughts
I often say that my mission isn't simply to help patients find clinical trials.
My mission is to help patients make informed decisions.
Those decisions begin long before someone signs a consent form.
They begin with understanding the unique biology of the cancer they're facing.
Because metastatic triple-negative breast cancer isn't one disease.
It never was.
It is heterogeneous.
And perhaps the most important question any patient can ask is not:
"What treatment should I receive?"
Instead, ask:
"Have we learned everything we can about my cancer before deciding what comes next?"
Karen's Club Takeaway
Know your diagnosis.
Know your biology.
Ask for the report.
Understand your options.
Make an informed decision.
Don't guess. Test.
Hugs.
K
sources cited: (1) ASCO Publications/ASCO Educational Book April 2026, (2) AACR’s Cancer Disparities Progress Report 2026
If you would like to discuss biomarker testing, the new mTNBC algorithm or clinical trials please feel free to schedule a free 1:1 patient consultation at https://www.karensclub.org/